

 Home
HomeReporting COVID deaths
Updated March 3, 2022
Behind every one of these statistics is an individual. We're saddened by every death and our hearts go out to the family and loved ones of these individuals who died.
DHSS is aware that the topic of how COVID-19 deaths are counted generates a great deal of interest. This webpage should answer some of your questions.
Current process
There are two avenues for the public reporting of COVID-19 deaths in Alaska.
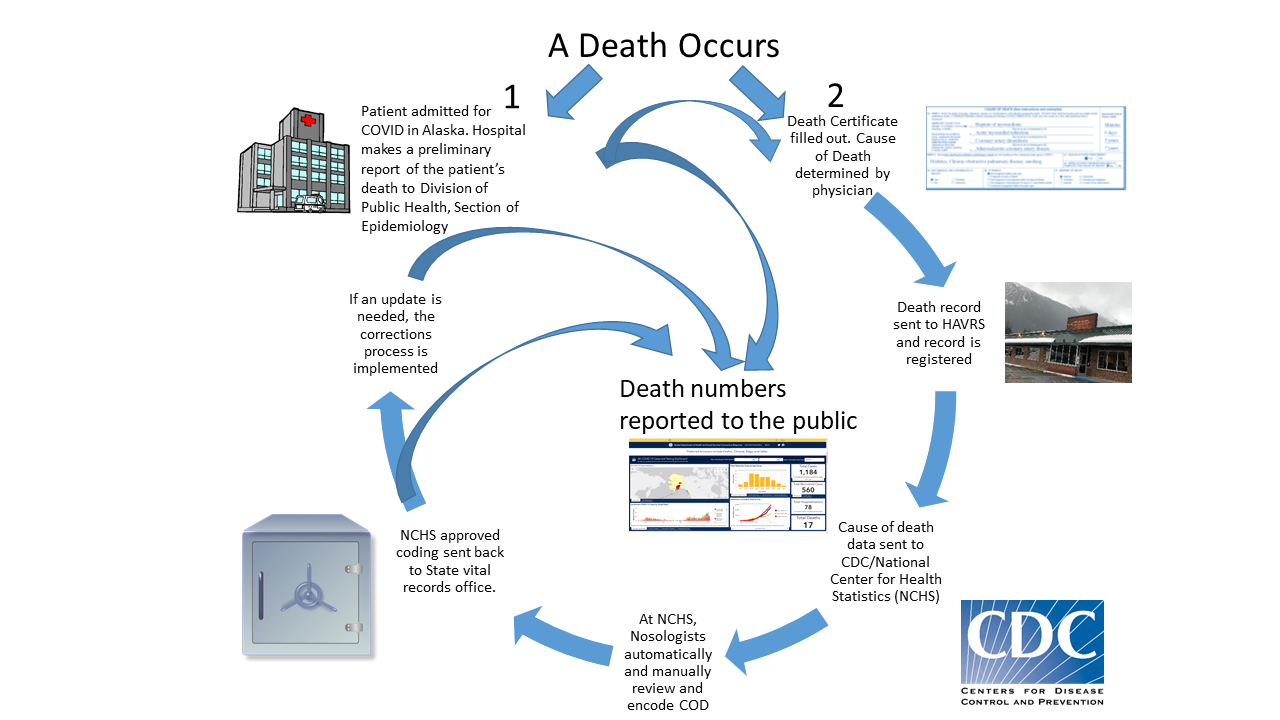
By health care facilities
The first is from reporting by health care facilities. Because COVID-19 is a reportable infectious condition, hospitals report cases of COVID-19 directly to the Division of Public Health's Sectison of Epidemiology. Later, if those hospitalized patients pass away, those deaths are also reported.
The benefit of this method is real time reporting. The state has the ability to report the death within days of the death occurring. However, this method may not capture deaths because of the time lag associated with COVID patients who may remain hospitalized for a longer period of time, have a more complex disease and death process, or died outside of Alaska. Further, this more real-time method means that deaths have not yet undergone review by CDC.
Through death certificates
The second process is through death certificates and their review by CDC. Every death in the state, and of out of state Alaska residents, results in the production of a death record. A death record contains the who, what, when, and where of a death. The cause of death section of a death record provides the 'why'. A death record is registered by the Division of Public Health's section of Health Analytics and Vital Records (HAVRS). The cause of death language is de-identified and forwarded to CDC's National Center for Health Statistics (NCHS). There the cause of death language is coded by nosologists (professional trained to classify disease) using the International Statistical Classification of Diseases and Related Health Problems (ICD-10) medical classification. Once coded, the data are sent back to HAVRS. These data essentially serve as the final cause of death description.
The benefit of reporting deaths that moved though the NCHS process is these data represent the most accurate death counts. The cause of death statements have undergone review and have been coded - coded as U07.1. However, a death certificate takes an average of 9 days from the death to be registered by the state. This is before the NCHS review. The disadvantage is a delay of one to three weeks for data review and return to the state. The data lag means NCHS provisional death counts may not reflect all deaths reported by the State during a given time period, especially for more recent periods.
Data corrections
Finally, data corrections may change death counts. On occasion a death record needs a correction that may change the death counts. An example might be the original death record had an incorrect state of residence. Generally, upon discovery, corrections are handled by a state's vital records office and the updated data are provided to NCHS if necessary.
The Death Certificate process
The federal government has worked with states to collect and standardize death reporting since the early 1900s. Cause of death and a decedent's demographics are first recorded onto a death record. Death records are administered by the vital records program in the state where the death occurred. A death record is first filled out by a funeral director; the cause of death section is provided by a medical professional; and final registration is completed by a state's vital records office.
CDC considers "Cause of Death" to be a best medical opinion. CDC wants the cause of death to come from medical professionals.
People can die from more than one cause. CDC reporting conventions allow a death certificates to capture the many conditions that contribute to a person's death. The Cause of Death section on a death certificate has two parts:
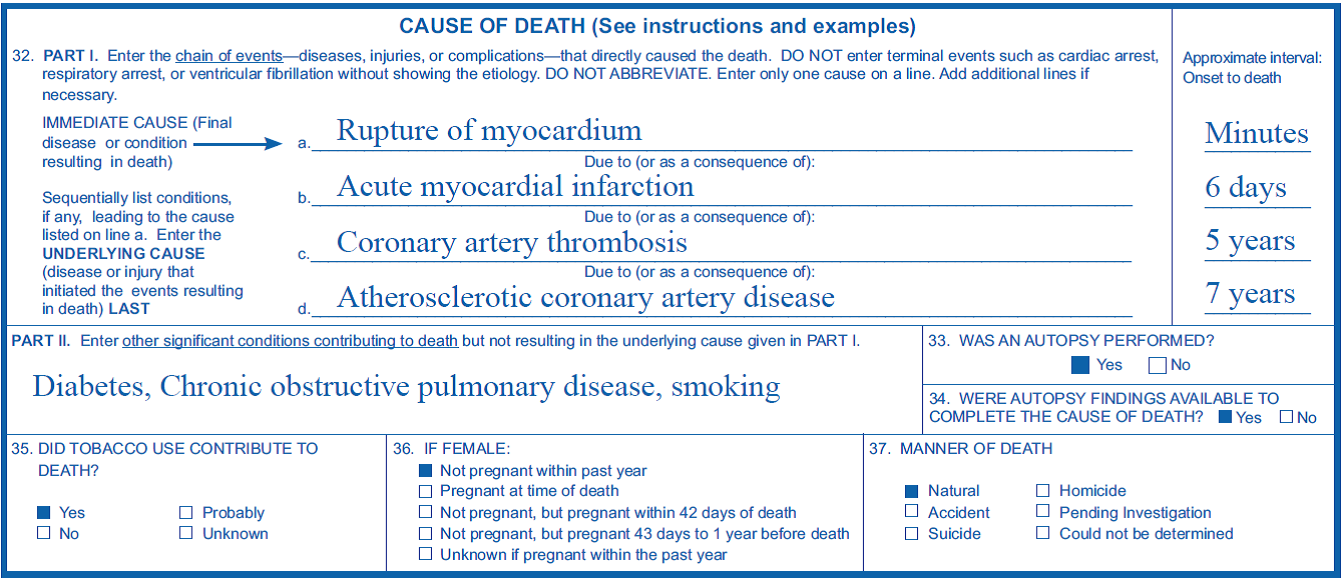
- Part I is the chain of events — the diseases, injuries, or conditions that directly cause the death. There are four lines available, 'a' through 'd'.
- Line 'a' is reserved for the immediate cause of death. The immediate cause of death is the final disease or condition that resulted in death.
- Line 'b' (and 'c' if necessary) are reserved for intermediate causes of death. The medical professional outlines the logical sequence of causes, or etiology that leads from the underlying cause of death to the immediate cause of death. Sometimes, there is no intermediate cause of death.
- The last line available is reserved for the underlying cause of death. This is the disease or injury that initiates the chain of events leading to the immediate cause of death.
- Part II is where a medical professional may enter any medical conditions that contributed or exacerbated, but did not cause, the death.
Note that for a death by a virus, if the symptomology and circumstances are compelling, and the medical professional is convinced a specific virus caused the death, NCHS will accept a cause of death certification without laboratory confirmation. Again, CDC is looking for a medical opinion. CDC does, however, encourage confirmation of viral deaths with testing.
After a death record has been certified, the cause of death section is forwarded to CDC's NCHS. NCHS nosologists review the data, determines its accuracy, electronically and manually code the deaths using ICD-10 classification, and report back the final and coded cause of death to the states. Nosology is a branch of medicine that deals with classification of disease. To become competent takes many years of training. This process has in place since the 1980s for all causes of death.
Dying from a condition versus dying with a condition
In the semantics of health researchers, dying from something means a condition is the underlying or contributing cause.
Consider the case in the example above. The immediate cause of death is a rupture of the myocardium, preceded by an intermediate cause acute myocardial infarction, preceded by an intermediate cause of coronary artery thrombosis, preceded by an underlying cause of atherosclerotic coronary artery disease. If a researcher were asked the cause of death for this individual, they would be correct to say either a rupture of the myocardium, a heart attack, a blocked artery, or hardening and narrowing of the arteries. If a researcher were performing a study on heart disease, this case would be counted. If a researcher were making an annual count of deaths from hardening and narrowing of the arteries in general, again this case would be included. On the other hand, if the researcher was developing a year-end report of leading causes of death, they would just report the underlying cause.
If a decedent had listed an immediate cause of death of stroke, that was a complication from an intermediate cause of blunt force trauma to the head, which had the underlying cause of a vehicle crash; a researcher would be correct in saying this individual died from a stroke, a head injury, or a car crash. Stroke and the head injury would be considered contributing causes associated with the underlying cause of a car crash.
On the other hand, if an individual died in a car crash also happen to test positive for COVID-19, COVID-19 would not be listed on the death certificate and the death would not be considered a COVID-19 death. This would be a case of dying with a disease. In this case, the death certificate would only list the sequence of conditions associated with the vehicle crash.
All reported Alaska resident COVID-19 deaths have the virus listed as a condition in Part I, Part II or the Injury Description. A death where COVID-19 is listed in Part II or the Injury Description might be considered as a contributing cause depending on how CDC nosologists interpret the cause of death provided by the medical professional. Most Alaskan deaths have listed COVID-19 somewhere in the lethal chain of conditions within Part I. However, if Alaska receives the U07.1 ICD-10 coding of a COVID-19 death from CDC, even from Part II or the Injury Description, we will report it.
Epidemiological significance of reporting COVID deaths
Whether COVID-19 shortened a life by 15 years or 15 minutes; whether COVID-19 is an underlying or contributing condition, the virus was in circulation, infected an Alaskan, and hastened their death. This must be reported.
Where can I find COVID Death Data?
You can find counts of COVID-19 deaths on the Alaska Coronavirus Response Hub: data.coronavirus.alaska.gov. On the COVID-19 Cases Dashboard, you can find the count of death that can be shown for Alaska residents (including AK residents diagnosed and isolated OOS), non-residents, or for both residents and non-residents diagnosed and isolated in Alaska. The "Cumulative Deaths" graph on the COVID-19 Cases Dashboard reflects the date when a death was confirmed by the State, not when the death occurred. "Table 1. Cases by Report Date" of the summary tables also shows a count of deaths; however, this table reflects deaths by the date when the case was confirmed COVID-19 positive, not by the date that the case was reported dead.